Neurocognitive mechanisms in compulsive sexual behavior disorder (2018) – Excerpts analyzing Prause et al., 2015
Link to PDF of full paper – Neurocognitive mechanisms in compulsive sexual behavior disorder (2018).
Excerpt analyzing Prause et al., 2015 (which is citation 87)
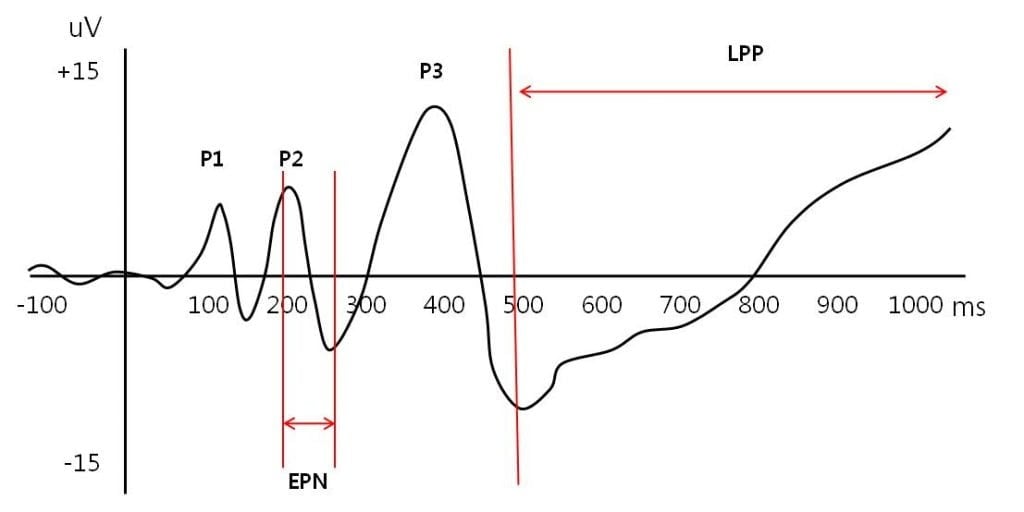
A study using EEG, conducted by Prause and colleagues, suggested that individuals who feel distressed about their pornography use, as compared to a control group who do not feel distress about their use of pornography, may require more/greater visual stimulation to evoke brain responses [87]. Hypersexual participants—individuals‘ experiencing problems regulating their viewing of sexual images’ (M=3.8 hours per week)—exhibited less neural activation (measured by late positive potential in the EEG signal) when exposed to sexual images than did the comparison group when exposed to the same images. Depending on the interpretation of sexual stimuli in this study (as a cue or reward; for more see Gola et al. [4]), the findings may support other observations indicating habituation effects in addictions [4]. In 2015, Banca and colleagues observed that men with CSB preferred novel sexual stimuli and demonstrated findings suggestive of habituation in the dACC when exposed repeatedly to the same images [88]. Results of the aforementioned studies suggest that frequent pornography use may decrease reward sensitivity, possibly leading to increased habituation and tolerance, thereby enhancing the need for greater stimulation to be sexually aroused. However, longitudinal studies are indicated to examine this possibility further. Taken together, neuroimaging research to date has provided initial support for the notion that CSB shares similarities with drug, gambling, and gaming addictions with respect to altered brain networks and processes, including sensitization and habituation.
COMMENTS: The authors of the current review agree with six other peer-reviewed papers (1, 2, 3, 4, 5, 6.): Lower EEG readings mean that subjects are paying less attention to the pictures. They were bored (habituated or desensitized). The lead author claims these results “debunk porn addiction”, but other researchers disagree with her over-the-top assertions. You have to ask yourself – “What legitimate scientist would claim that their lone anomalous study has debunked a well established field of study?”
- Prause N, Steele VR, Staley C, Sabatinelli D, Proudfit GH. Modulation of late positive potentials by sexual images in problem users and controls inconsistent with “porn addiction”. Biol Psychol. 2015;109:192-9.
Abstract
Purpose of review: The current review summarizes the latest findings concerning neurobiological mechanisms of compulsive sexual behavior disorder (CSBD)and provides recommendations for future research specific to the diagnostic classification of the condition.
Recent findings: To date, most neuroimaging research on compulsive sexual behavior has provided evidence of overlapping mechanisms underlying compulsive sexual behavior and non-sexual addictions. Compulsive sexual behavior is associated with altered functioning in brain regions and networks implicated in sensitization, habituation, impulse dyscontrol, and reward processing in patterns like substance, gambling, and gaming addictions. Key brain regions linked to CSB features include the frontal and temporal cortices, amygdala, and striatum, including the nucleus accumbens.
Summary: Despite much neuroscience research finding many similarities between CSBD and substance and behavioral addictions, the World Health Organization included CSBD in the ICD-11 as an impulse-control disorder. Although previous research has helped to highlight some underlying mechanisms of the condition, additional investigations are needed to fully understand this phenomenon and resolve classification issues surrounding CSBD.
Introduction
Compulsive sexual behavior (CSB) is a debated topic that is also known as sexual addiction, hypersexuality, sexual dependence, sexual impulsivity, nymphomania, or out-of-control sexual behavior [1-27]. Although precise rates are unclear given limited epidemiological research, CSB is estimated to affect 3-6% of the adult population and is more common in men than women [28-32]. Due to the associated distress and impairment reported by men and women with CSB [4-6, 30, 33-38], the World Health Organization (WHO) has recommended including Compulsive Sexual Behavior Disorder(CSBD)in the forthcoming 11th edition of the International Classification of Diseases (6C72)[39]. This inclusion should help increase access to treatment for unserved populations, reduce stigma and shame associated with help-seeking, promote concerted research efforts, and increase international attention on this condition[40, 41].We acknowledge that over the last 20 years there have been varying definitions used to describe dysregulated sexual behaviors often characterized by excessive engagement in nonparaphilic sexual activities (e.g., frequent casual/anonymous sex, problematic use of pornography). For the current review, we will use the term CSB as an overarching term for describing problematic, excessive sexual behavior.
CSB has been conceptualized as an obsessive–compulsive-spectrum disorder, an impulse-control disorder, or addictive behavior [42, 43]. The symptoms of CSBD are like those proposed in 2010forthe DSM-5 diagnosis of hypersexual disorder [44]. Hypersexual disorder was ultimately excluded by American Psychiatric Association from DSM-5 for multiple reasons; the lack of neurobiological and genetic studies was among the most noted reasons [45, 46]. More recently, CSB has received considerable attention in both popular culture and social sciences, particularly given health disparities affecting at-risk and underserved groups. Despite the considerable increase in studies of CSB (including those studying “sexual addiction,” “hypersexuality,” “sexual compulsivity”), relatively little research has examined neural underpinnings of CSB [4, 36]. This article reviews neurobiological mechanisms of CSB and provides recommendations for future research, particularly as related to diagnostic classification of CSBD.
CSB as an Addictive Disorder
Brain regions involved in processing rewards are likely important for understanding the origins, formation, and maintenance of addictive behaviors [47]. Structures within a so-called ‘reward system’ are activated by potentially reinforcing stimuli, such as addictive drugs in addictions. A major neurotransmitter involved in processing rewards is dopamine, particularly within the mesolimbic pathway involving the ventral tegmental area (VTA) and its connections with the nucleus accumbens (NAc), as well as the amygdala, hippocampus, and prefrontal cortex [48]. Additional neurotransmitters and pathways are involved in processing rewards and pleasure, and these warrant considerations given that dopamine has been implicated to varying degrees in individual drug and behavioral addictions in humans [49-51].
According to the incentive salience theory, different brain mechanisms influence motivation to obtain reward (‘wanting’) and the actual hedonic experience of reward (‘liking’) [52]. Whereas ‘wanting’ may be closely related to dopaminergic neurotransmission in the ventral striatum (VStr) and orbitofrontal cortex, networks dedicated to creating wanting motivations and pleasurable feelings are more complex [49, 53, 54].
VStr reward-related reactivity has been studied in addictive disorders such as alcohol, cocaine, opioid use disorders, and gambling disorder[55-58]. Volkow and colleagues describe four important components of addiction: (1) sensitization involving cue reactivity and craving, (2) desensitization involving habituation, (3) hypofrontality, and (4) malfunctioning stress systems[59]. Thus far, research of CSB has largely focused on cue reactivity, craving, and habituation. The first neuroimaging studies of CSB were focused on examining potential similarities between CSB and addictions, with a specific focus on the incentive salience theory that is based on preconscious neural sensitization related to changes in dopamine-related motivation systems[60]. In this model, repeated exposure to potentially addictive drugs may change brain cells and circuits that regulate the attribution of incentive salience to stimuli, which is a psychological process involved in motivated behavior. Because of this exposure, brain circuits may become hypersensitive (or sensitized), thereby contributing to the development of pathological levels of incentive salience for target substances and their associated cues. Pathological incentive motivation (‘wanting’) for drugs may last for years, even if drug use is discontinued. It may involve implicit (unconscious wanting) or explicit (conscious craving) processes. The incentive salience model has been proposed to potentially contribute to the development and maintenance of CSB [1, 2].
Data support the incentive salience model for CSB. For example, Voon and colleagues examined cue-induced activity in the dorsal anterior cingulate cortex (dACC) –Vstr –amygdala functional network [1].Men with CSB as compared to those without showed increased VStr, dACC, and amygdala responses to pornographic video clips. These findings in the context of the larger literature suggest that sex and drug-cue reactivity involve largely overlapping regions and networks[61, 62]. Men with CSB as compared to those without also reported higher wanting (subjective sexual desire) of pornography stimuli and lower liking which is consistent with an incentive salience theory[1]. Similarly, Mechelmans and colleagues found that men with CSB as compared to men without showed enhanced early attentional bias towards sexually explicit stimuli but not to neutral cues [2]. These findings suggest similarities in enhanced attentional bias observed in studies examining drug cues in addictions.
In 2015, Seok and Sohn found that among men with CSB as compared to those without, greater activity was observed in the dorsolateral prefrontal cortex (dlPFC), caudate, inferior supramarginal gyrus of the parietal lobe, dACC, and thalamus in response to sexual cues[63]. They also found that the severity of CSB symptoms was correlated with cue-induced activation of the dlPFC and thalamus. In 2016, Brand and colleagues observed greater activation of the VStr for preferred pornographic material as compared to non-preferred pornographic material among men with CSB and found that VStr activity was positively associated with self-reported symptoms of addictive use of Internet pornography (assessed by the short Internet Addiction Test modified for cybersex (s-IATsex) [64, 65].
Klucken and colleagues recently observed that participants with CSB as compared to participants without displayed greater activation of the amygdala during presentation of conditioned cues (colored squares) predicting erotic pictures (rewards) [66]. These results are like those from other studies examining amygdala activation among individuals with substance use disorders and men with CSB watching sexually explicit video clips [1, 67].Using EEG, Steele and colleagues observed a higher P300 amplitude to sexual images (when compared to neutral pictures) among individuals self-identified as having problems with CSB, resonating with prior research of processing visual drug cues in drug addiction [68, 69].
In 2017, Gola and colleagues published results of a study using functional magnetic resonance imaging (fMRI) to examine Vstr responses to erotic and monetary stimuli among men seeking treatment for CSB and men without CSB [6]. Participants were engaged in an incentive delay task[54, 70, 71] while undergoing fMRI scanning. During this task, they received erotic or monetary rewards preceded by predictive cues. Men with CSB differed from those without in VStr responses to cues predicting erotic pictures, but not in their responses to erotic pictures. Additionally, men with CSB versus without CSB showed greater VStr activation specifically for cues predicting erotic pictures and not for those predicting monetary rewards. Relative sensitivity to cues (predicting erotic pictures vs. monetary gains) was found to be related to an increased behavioral motivation for viewing erotic images (‘wanting’), intensity of CSB, amount of pornography used per week, and frequency of weekly masturbation. These findings suggest similarities between CSB and addictions, an important role for learned cues in CSB, and possible treatment approaches, particularly interventions focused on teaching skills to individuals to successfully cope with cravings/urges [72]. Furthermore, habituation may be revealed through decreased reward sensitivity to normally salient stimuli and may impact reward responses to sexual stimuli including pornography viewing and partnered sex [1, 68]. Habituation has also been implicated in substance and behavioral addictions [73-79].
In 2014, Kuhn and Gallinat observed decreased VStr reactivity in response to erotic pictures in a group of participants watching pornography frequently, when compared to participants watching pornography rarely[80].Decreased functional connectivity between the left dlPFC and right VStr was also observed. Impairment in fronto-striatal circuity has been related to inappropriate or disadvantageous behavioral choices irrespective of potential negative outcome and impaired regulation of craving in drug addiction [81, 82]. Individuals with CSBmay have reduced executive control when exposed to pornographic material [83, 84]. Kuhn and Gallinat also found that the gray matter volume of the right striatum(caudate nucleus), which has been implicated in approach-attachment behaviors and related to motivational states associated with romantic love, was negatively associated with duration of internet pornography viewing[80, 85, 86]. These findings raise the possibility that frequent use of pornography may decrease brain activation in response to sexual stimuli and increase habituation to sexual pictures although longitudinal studies are needed to exclude other possibilities.
A study using EEG, conducted by Prause and colleagues, suggested that individuals who feel distressed about their pornography use, as compared to a control group who do not feel distress about their use of pornography, may require more/greater visual stimulation to evoke brain responses [87]. Hypersexual participants—individuals‘ experiencing problems regulating their viewing of sexual images’ (M=3.8 hours per week)—exhibited less neural activation (measured by late positive potential in the EEG signal) when exposed to sexual images than did the comparison group when exposed to the same images. Depending on the interpretation of sexual stimuli in this study (as a cue or reward; for more see Gola et al. [4]), the findings may support other observations indicating habituation effects in addictions [4].In 2015, Banca and colleagues observed that men with CSB preferred novel sexual stimuli and demonstrated findings suggestive of habituation in the dACC when exposed repeatedly to the same images [88]. Results of the aforementioned studies suggest that frequent pornography use may decrease reward sensitivity, possibly leading to increased habituation and tolerance, thereby enhancing the need for greater stimulation to be sexually aroused. However, longitudinal studies are indicated to examine this possibility further. Taken together, neuroimaging research to date has provided initial support for the notion that CSB shares similarities with drug, gambling, and gaming addictions with respect to altered brain networks and processes, including sensitization and habituation.
CSB as an Impulse-Control Disorder?
The category of “Impulse-Control Disorders Not Elsewhere Classified” in DSM-IV was heterogeneous in nature and included multiple disorders that have since been re-classified as being addictive (gambling disorder) or obsessive-compulsive-related (trichotillomania) in DSM-5[89, 90]. The current category in the DSM-5 focuses on disruptive, impulse-control and conduct disorders, becoming more homogeneous in its focus by including kleptomania, pyromania, intermittent explosive disorder, oppositional defiant disorder, conduct disorder, and antisocial personality disorder[90]. The category of impulse-control disorders in the ICD-11includes these first three disorders and CSBD, raising questions regarding the most appropriate classification. Given this context, how CSBD relates to the transdiagnostic construct of impulsivity warrants additional consideration for classification as well as clinical purposes.
Impulsivity may be defined as a, “predisposition towards rapid, unplanned reactions to internal or external stimuli with diminished regard to the negative consequences to the impulsive individual or others” [91]. Impulsivity has been associated with hypersexuality [92]. Impulsivity is a multidimensional construct with different types (e.g., choice, response) that may have trait and state characteristics [93-97]. Different forms of impulsivity may be assessed via self-report or via tasks. They may correlate weakly or not all, even within the same form of impulsivity; importantly, they may relate differentially to clinical characteristics and outcomes [98]. Response impulsivity maybe measured by performance on inhibitory control tasks, such as the stop signal or Go/No-Go tasks, whereas choice impulsivity may be assessed through delay discounting tasks [94, 95, 99].
Data suggest differences between individuals with and without CSB on self-report and task-based measures of impulsivity [100-103]. Furthermore, impulsivity and craving seem to be associated with the severity of symptoms of dysregulated pornography use, such as loss of control [64, 104]. For instance, one study found interacting effects of levels of impulsivity measured by self-report and behavioral tasks with respect to cumulative influences on symptom severity of CSB [104].
Among treatment-seeking samples, 48% to 55% of people may exhibit high levels of generalized impulsivity on Barratt Impulsiveness Scale [105-107]. In contrast, other data suggest that some patients seeking treatment for CSB do not have other impulsive behaviors or comorbid addictions beyond their struggles with sexual behaviors which is consistent with findings from a large online survey of men and women suggesting relatively weak relations between impulsivity and some aspects of CSB (problematic pornography use) and stronger relations with others (hypersexuality) [108, 109]. Similarly, in a study using different measures of individuals with problematic pornography use(mean time of weekly pornography use = 287.87 minutes) and those without (mean time of weekly pornography use = 50.77 minutes) did not differ on self-reported (UPPS-P Scale) or task-based (Stop Signal Task)measures of impulsivity [110].Further, Reid and colleagues did not observe differences between individuals with CSB and healthy controls on neuropsychological tests of executive functioning (i.e., response inhibition, motor speed, selective attention, vigilance, cognitive flexibility, concept formation, set shifting),even after adjusting for cognitive ability in analyses [103]. Together, findings suggest that impulsivity may link most strongly to hypersexuality but not to specific forms of CSB like problematic pornography use. It raises questions about CSBD’s classification as an impulse-control disorder in the ICD-11 and highlights the need for precise assessments of different forms of CSB. This is particularly important since some research indicates that impulsivity and subdomains of impulse-control disorder differ on conceptual and pathophysiological level [93, 98, 111].
CSB as an Obsessive-Compulsive-Spectrum Disorder?
One condition (trichotillomania) classified as an impulse-control disorder in DSM-IV has been reclassified with obsessive-compulsive disorder (OCD) as an obsessive-compulsive and related disorder in DSM-5[90]. Other DSM-IV impulse-control disorders like gambling disorder exhibit significant differences from OCD, supporting their classification in separate categories [112]. Compulsivity is a transdiagnostic construct that involves, “the performance of repetitive and functionally impairing overt or covert behavior without adaptive function, performed in a stereotyped or habitual fashion, either according to rigid rules or as a means to avoid negative consequences”[93]. OCD exhibits high levels of compulsivity; however, so do substance addictions and behavioral addictions like gambling disorder [98]. Traditionally, compulsive and impulsive disorders were construed as lying along opposite ends of a spectrum; however, data suggest the constructs as being orthogonal with many disorders scoring high on measures of both impulsivity and compulsivity [93, 113]. Regarding CSB, sexual obsessions have also been described as time-consuming and interfering and may relate theoretically to OCD or to OCD-related features [114].
Recent studies assessing obsessive-compulsive features using the Obsessive-Compulsive Inventory –Revised (OCI-R) did not show elevations among individuals with CSB [6, 37, 115]. Similarly, a large online survey found aspects of compulsivity only weakly related to problematic pornography use[109]. Together, these findings do not show strong support for considering CSB as an obsessive-compulsive-related disorder. Neural features underlying compulsive behaviors have been described and overlap across multiple disorders [93]. Further studies using psychometrically validated and neuroimaging methods in larger clinical treatment seeking samples are needed to examine further how CSBD may relate to compulsivity and OCD.
Structural Neural Changes among CSB Individuals
Thus far, most neuroimaging studies have focused on functional alterations in individuals with CSB, and results suggest that CSB symptoms are linked to specific neural processes[1, 63, 80]. Although task-based studies have deepened our knowledge about regional activation and functional connectivity, additional approaches should be used.
White-or gray-matter measures have been studied in CSB [102, 116]. In 2009, Miner and colleagues found that individuals with CSB as compared to those without displayed higher superior frontal region mean diffusivity and exhibited poorer inhibitive control. In a study of men with and without CSB from 2016, greater left amygdala volume was observed in the CSB group and relatively reduced resting-state functional connectivity was observed between the amygdala and dlPFC [116]. Reduction of brain volumes in the temporal lobe, frontal lobe, hippocampus, and amygdala were found to be related to the symptoms of hypersexuality in patients with dementia or Parkinson’s disease [117, 118]. These seemingly opposing patterns of amygdala volume relating to CSB highlight the importance of considering co-occurring neuropsychiatric disorders in understanding the neurobiology of CSB.
In 2018, Seok and Sohn used voxel-based morphometry (VBM) and resting-state connectivity analysis to examine gray-matter and resting-state measures in CSB [119]. Men with CSB showed significant gray-matter reduction in the temporal gyrus. Left superior temporal gyrus (STG) volume was negatively correlated with the severity of CSB (i.e., Sexual Addiction Screening Test-Revised [SAST ] and Hypersexual Behavior Inventory [HBI] scores)[120, 121]. Additionally, altered left STG-left precuneus and left STG-right caudate connectivities were observed. Lastly, results revealed a significant negative correlation between severity of CSB and functional connectivity of the left STG to the right caudate nucleus.
While the neuroimaging studies of CSB have been illuminating, little is still known about alternations in brain structures and functional connectivity among CSB individuals, particularly from treatment studies or other longitudinal designs. Integration of findings from other domains (e.g., genetic and epigenetic) will also be important to consider in future studies. Additionally, findings directly comparing specific disorders and incorporating transdiagnostic measures will allow for collection of important information that could inform classification and intervention development efforts currently underway.
Conclusions and Recommendations
This article reviews scientific knowledge regarding neural mechanisms of CSB from three perspectives: addictive, impulse-control, and obsessive-compulsive. Several studies suggest relationships between CSB and increased sensitivity for erotic rewards or cues predicting these rewards, and others suggest that CSB is related to increased cue-conditioning for erotic stimuli [1, 6, 36, 64, 66]. Studies also suggest that CSB symptoms are associated with elevated anxiety [34, 37,122]. Although gaps exist in our understanding of CSB, multiple brain regions (including frontal, parietal and temporal cortices, amygdala, and striatum) have been linked to CSB and related features.
CSBD has been included in the current version oftheICD-11as an impulse-control disorder [39]. As described by the WHO, ‘Impulse-control disorders are characterized by the repeated failure to resist an impulse, drive, or urge to perform an act that is rewarding to the person, at least in the short-term, despite consequences such as longer-term harm either to the individual or to others, marked distress about the behaviour pattern, or significant impairment in personal, family, social, educational, occupational, or other important areas of functioning’ [39]. Current findings raise important questions regarding the classification of CSBD. Many disorders characterized by impaired impulse-control are classified elsewhere in the ICD-11 (for example, gambling, gaming, and substance-use disorders are classified as being addictive disorders) [123].
Currently, CSBD constitutes a heterogeneous disorder, and further refinement of CSBD criteria should distinguish between different subtypes, some of which may relate to the heterogeneity of sexual behaviors problematic for individuals [33, 108, 124]. Heterogeneity in CSBD may in part explain seeming discrepancies which are noticeable across studies. Although neuroimaging studies find multiple similarities between CSB and substance and behavioral addictions, additional research is needed to fully understand how neurocognition relates to the clinical characteristics of CSB, especially with respect to sexual behaviors subtypes. Multiple studies have focused exclusively on problematic use of pornography which may limit generalizability to other sexual behaviors. Further, inclusion/exclusion criteria for CSB research participants have varied across studies, also raising questions regarding generalizability and comparability across studies.
Future Directions
Several limitations should be noted with respect to current neuroimaging studies and be considered when planning future investigations (see Table 1). A primary limitation involves small sample sizes that are largely white, male, and heterosexual. More research is needed to recruit larger, ethnically diverse samples of men and women with CSB and individuals of different sexual identities and orientations. For example, no systematic scientific studies have investigated neurocognitive processes of CSB in women. Such studies are needed given data linking sexual impulsivity to greater psychopathology in women as compared to men and other data which suggest gender-related differences in clinical populations with CSB [25, 30]. As women and men with addictions may demonstrate different motivations (e.g., relating to negative versus positive reinforcement) for engaging in addictive behaviors and show differences in stress and drug-cue responsivity, future neurobiological studies should consider stress systems and related processes in gender-related investigations of CSBD given its current inclusion in the ICD-11 as a mental health disorder [125, 126].
Similarly, there is also a need to conduct systematic research focusing on ethnic and sexual minorities to clarify our understanding of CSB among these groups. Screening instruments for CSB have been mostly tested and validated on white European men. Moreover, current studies have focused predominantly on heterosexual men. More research examining clinical characteristics of CSB among gay and bisexual men and women is needed. Neurobiological research of specific groups (transgender, polyamorous, kink, other) and activities (pornography viewing, compulsive masturbation, casual anonymous sex, other) is also needed. Given such limitations, existing results should be interpreted cautiously.
Direct comparison of CSBD with other disorders (e.g., substance use, gambling, gaming, and other disorders)is needed, as is incorporation of other non-imaging modalities (e.g., genetic, epigenetic) and use of other imaging approaches. Techniques like positron emission tomography could also provide important insight into neurochemical underpinnings of CSBD.
The heterogeneity of CSB may also be clarified through careful assessment of clinical features that may be obtained in part from qualitative research like focus group ordiary assessment methods [37]. Such research could also provide insight into longitudinal questions like whether problematic pornography use may lead to sexual dysfunction, and integrating neurocognitive assessments into such studies could provide insight into neurobiological mechanisms. Further, as behavioral and pharmacological interventions are formally tested for their efficacies in treating CSBD, integration of neurocognitive assessments could help identify mechanisms of effective treatments for CSBD and potential biomarkers. This last point may be particularly important because the inclusion of CSBD in the ICD-11 will likely increase the number of individuals seeking treatment for CSBD. Specifically, the inclusion of CSBD in the ICD-11 should raise awareness in patients, providers, and others and potentially remove other barriers (e.g., reimbursement from insurance providers) that may currently exist for CSBD.